
Orthodox Budget and Hot off the Fire Challenges in the Health Sector of Bangladesh
Tahia Anan Dhira
HERN member and Lecturer, Department of Economics, University of Dhaka
Despite its many achievements, Bangladesh’s health system faces multiple hurdles, and it appears still to receive adequate attention in terms of national resource allocation. Every year the amount of money allocated in the budget for health is increased compared to the prior fiscal year. Thanks to the government for the raise. However, it is also very obvious that the mark up would be a trifling sum. This year it was the same as COVID – 19 debacle failed to enunciate the healthcare sector’s budget objectives. The national budget for FY 2022-23 appears similar to the recent years, as only 5.43 percent of the entire budget is allotted to the health sector. In FY 2021 – 22, the share of the budget in the health sector was 5.15 percent, which was 4.72 percent in the previous fiscal year. While the overall budget increased by 14.24 percent for FY 2022-2023, the minister only allowed a 12.62 percent uptick for the health sector, which is not startling. This fiscal year’s allocation for the health sector is Tk 36,864 crore, up against Tk 32,731 crore last year(1).
Additionally, the projected allotment for the Medical Education and Family Welfare Division (MEFWD) will be Tk 7,582 crore, up from Tk 6,110 crore in the previous fiscal year. However, the provision for the health services division is meager. For the upcoming fiscal year, the finance minister has requested Tk 29,282 crore for the health service division, up from Tk 26,165 crore in the previous fiscal year(2). The Integrated Health Science Research and Development Fund’s budget stays unchanged at Tk 100 crore.
Also, the government had set aside TK 10,000 crore in the last two fiscal years’ budgets to meet urgent health sector demand during the country’s COVID – 19 outbreak. However, in this new fiscal year, this amount will be reduced and only TK 5,000 crore has been designated to address the urgent demand(1). As a result, experts are voicing concerns about how this budget would ensure emergency medical services, especially during epidemics.

Experts have also specified that there is nothing novel in this year’s budget that will aid in restructuring the health-care system, as there will be no mega plan and no long-term and sustainable investments in the management of coronaviruses and other infectious diseases. Only short-term and immediate demands will be fulfilled with the current allocation.

Bangladesh’s public healthcare budget is among the lowest in the world, resulting in significant underinvestment in public healthcare facilities. Bangladesh spends an estimated 2.3 percent of its GDP on current health expenditure (CHE), the lowest in the South Asian region (3). It has a per-capita annual CHE of roughly $45, compared to $58 in Nepal, $73 in India, $103 in Bhutan, and $157 in Sri Lanka. Experts suggested giving 7 to 8 percent of the budget to the health sector in FY 2022-23.
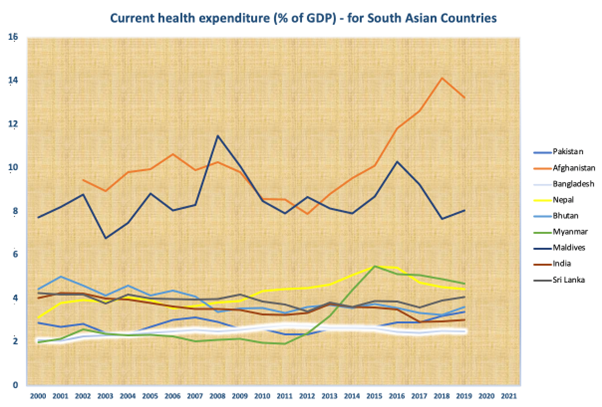
Source: The World Bank
Furthermore, when it comes to allocating health budgets, primary healthcare is consistently underestimated. We have felt the anguish of a shortage of inpatient beds, critical care beds, diagnostic facilities, oxygen, the presence, and adequacy of doctors in healthcare facilities across the country, and public awareness during the COVID-19 pandemic (4). In essence, we have realized how defenseless our healthcare system is in an emergency. Primary healthcare typically receives 25 percent of health-sector funding. This figure should be increased to 30 percent in the coming fiscal year, and in the medium term, it should be raised to 35-40 percent (2). Experts have also proposed forming a national commission to ensure that primary healthcare is of high quality (5). Their proposals, however, are not reflected in the budget this year.
Likewise, before the pandemic, Bangladesh’s leading health concern was non-communicable diseases (NCDs), which were responsible for 67 percent of the country’s deaths. By 2030, the country aims to reduce NCD-related deaths by one-third. However, the policies place a greater emphasis on paperwork than on effective implementation mechanisms. Primary healthcare facilities are not equipped to deal with NCDs, and the District Health Information Software (DHIS2) has yet to collect data on associated service provision. This deficiency is not underscored even in this budget.
Even though increasing the allocation in the health sector is critical, the government will not be able to do so rapidly. The reason may lie behind the public health authorities’ lack of capacity to utilize the budget allocation effectively. According to the Implementation Monitoring and Evaluation Division (IMED) of the government, the health sector is the poorest performer among the top 15 ministries when it comes to implementing the Annual Development Program (ADP) (6). The Ministry of Health and Family Welfare (MOHFW) has not grown capacity to use up even three- fourth of the Annual Development Program (ADP) budget. On top of it, due to complex bureaucratic procedures, the allotted 100 crore for research and development remains under-utilized(6) .
Moreover, the MOHFW announced the Healthcare Financing Strategy (HCFS) 2012-2032, intending to halve the rate of out-of-pocket (OOP) spending. The government estimated OOP healthcare expenditure as a percentage of Total Health Expenditure (THE) was 67 percent (BNHA, 2015), and the World Bank estimated OOP healthcare expenditure as a percentage of Current Health Expenditure (CHE) was 71.82 percent (WB, 2015). However, the OOP payment is increasing with time. Now, it has grown to 72.7 percent of CHE (WB, 2019), which is also one of the lowest in South Asia. OOP healthcare expenditure pushes nearly 4.2 percent of the population yearly (5.8 million people) to extreme poverty (7). In the face of rising inequality, the top quintile spends on average seven times more than the bottom quintile. The wealthiest quintile of Bangladesh’s population pays most of OOP funding to the country’s healthcare system due to the high relationship between OOP health spending and household income. They spend 40-42 percent of all OOP spending, which is significantly more than the bottom 60 percent (8). As a result, even if reducing OOP health expenditure is a lengthy concern, it may be possible to reduce the costs faced by the poor. The absence of clear guidelines to reduce OOP healthcare expenditure in this budget is startling.
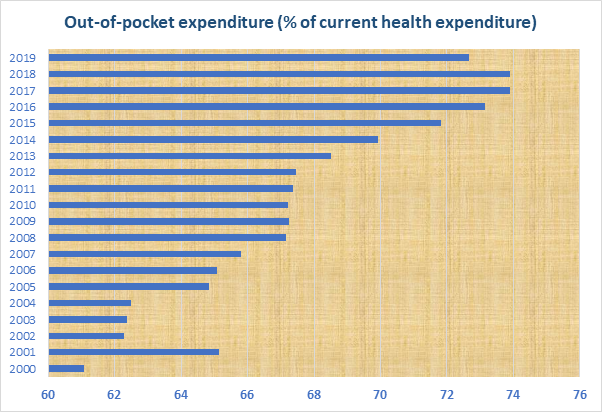
Source: The World Bank
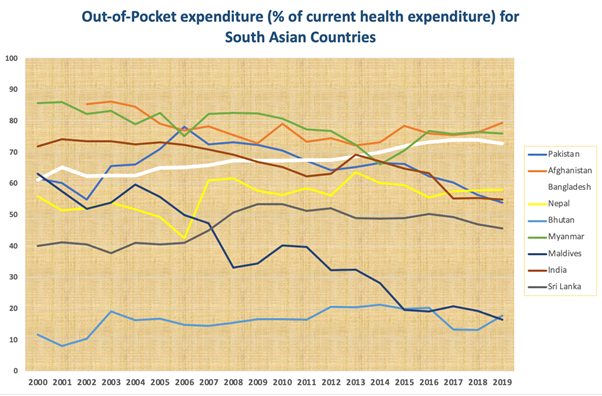
Source: The World Bank
Likewise, the government has also committed to achieving Universal Health Coverage (UHC), which means that everyone has access to the health services they need, when and where they need them, without facing financial hardship. This is also the target 3.8 of the Sustainable Development Goals (SDGs) to be met by 2030. As a nation, we have not yet envisioned the strategies to achieve UHC. By definition, UHC incorporates all three (primary, secondary, and tertiary) stages of the country’s healthcare system. With an objective to the success of this target, we are proposing a community clinic model here to ensure UHC by 2041.
This model proposes a referral path to secondary and tertiary healthcare, commencing with primary care in community clinics. All community clinics will have enough physicians, nurses, and also laboratory experts who will be responsible to the Directorate General of Health Services (DGHS), the Directorate General of Nursing and Midwifery (DGNM), and the Directorate General of Laboratory Medicines (DGLM) respectively. Though Bangladesh already has DGHS and DGNM, it is yet to formulate DGLM. Essential Drugs Company Limited (EDCL) is yet to make sophisticated and costly medicines like cancer drugs etc. We must increase EDCL’s capacity by 2041 in order for it to be able to produce all advanced medications at its facility. For a set payment, it will offer the clinics access to medications. Thus, all kinds of medicine will be affordable and available throughout the country. Anywhere around the country, if a person falls sick or comes across an accident, they will be taken to the nearest hospital. The hospital will be capable of diagnosing the condition and its severity, as there will be a diagnostic lab and technicians. Primary treatment will be given by the present doctors and nurses. If the patient requires complex treatment, they will be referred by the clinic doctors to the district-level hospitals or other tertiary healthcare centers. This model could be comprehensive by including biosecurity issues, which may enable our healthcare system to comply with the ‘One Health Program’ of the World Health Organization (WHO). Focusing solely on human health while other living beings are infected with new types of microorganisms will not ensure our sustained wellness, as we share the same eco-system and are readily infected by one another’s diseases (9). Hence, we must also consider animal health issues in order to develop a long-term health strategy.
The biopharmaceutical industry in Bangladesh is now in its infancy, owing to private enterprises’ profit-driven culture and a scarcity of well-trained workers. Rather than relying on highly paid experts from other nations, local life sciences graduates can be trained. If a quality benchmark is established from the start, EDCL may not only develop these pharmaceuticals in a public-private partnership model to suit the country’s needs but also export them abroad. The scientific competence of EDCL must be rapidly enhanced in order to achieve such an ambitious objective.
Clearly, when it comes to removing the everlasting health sector problems in Bangladesh, everything boils down to bolstering human resources in this sector. Currently, we have an enormous shortage of doctors, nurses, and lab technicians (10). Lack of incentives, absence of coordination, and bureaucratic complexity to adopt and monitor policies come next. Therefore, to achieve UHC, the government needs to immediately take a mega plan and recalibrate the budgetary allotment for the health sector accordingly. As the country’s demographic dividend changes, a more extensive healthcare system will be required to support the aging population. In order to reduce OOP healthcare expenditure and achieve UHC, the health sector must expand fiscally. Reduced inefficiencies and improved capacity to proficiently spend the given public funding are just as crucial as increasing allotment. We will get smacked with health shocks from time to time unless and until we come up with a comprehensive strategy to meet healthcare goals and other challenges highlighted therein, and we already know how fragile we are to sudden catastrophe.
Reference
1. Budget FY23: Health sectors gets 36,863C. Dhaka Tribune. 2022 Jun 9;
2. National Budget Speech 2022-23. Dhaka: Ministry of Finance, Government of the People’s Republic of Bangladesh; Jun 11, 2022 p. 54–5.
3. Raise health allocation to 30pc. The Financial Express. 2022 May 13;
4. Khatun F. Expectations for the health sector in a pandemic budget. The Daily Star. 2021 May 31;
5. FY 2022-23: “Allocate 5 to 6pc of total budget for health sector.” The Daily Prothom Alo. 2022 May 12;
6. Huque R, Hasan T. Health sector must focus more on budget implementation. The Financial Express. 2021 Jul 8;
7. Huq NM, Al-Amin AQ, Howlader SR, Kabir MA. Paying out of pocket for healthcare in Bangladesh – A burden on poor? Vol. 44, Iranian Journal of Public Health. 2015.
8. Rezvi MR, Hossain MR. Health Financing in Bangladesh: Scarcity and its Impacts. SSRN Electronic Journal. 2022;
9. Lebov J, Grieger K, Womack D, Zaccaro D, Whitehead N, Kowalcyk B, et al. A framework for One Health research. Vol. 3, One Health. 2017.
10. Razu SR, Yasmin T, Arif TB, Islam MS, Islam SMS, Gesesew HA, et al. Challenges Faced by Healthcare Professionals During the COVID-19 Pandemic: A Qualitative Inquiry From Bangladesh. Frontiers in Public Health. 2021;